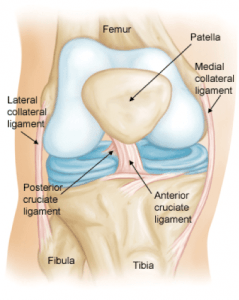
Anterior Cruciate Ligaments (ACL)
Anterior cruciate ligament ruptures are a relatively common injury, especially in sports that involve changing direction whilst running. The anterior cruciate ligament prevents the tibia from moving forwards on the femur and also provides rotational stability.
Treatment may be nonsurgical or surgical, depending on your desired lifestyle. The question is not so much your level of activity in the past, but expectations for the future. Sedentary people and recreational athletes who are prepared to modify their activities to avoid further knee problems may opt for conservative nonsurgical treatment.
However, if your goal is to continue an active lifestyle, surgery may be the treatment of choice because a torn ACL does not heal.
The goals of surgery are to:
- Stabilise the knee and prevent further episodes of giving way thereby reducing the risk of further meniscal and cartilage damage.
- Allow the patient to return to an active lifestyle and be able to participate in “cutting” sports (sports where a change in direction is needed i.e. rugby, football, netball etc.)
BEFORE SURGERY
The surgery is done as day surgery, so you will be admitted to the hospital 2 hours before your surgery is planned and go home the same day about 2 hours post surgery.
You will be required to have nothing to eat or drink for at least six hours before your surgery. You will be admitted to a bed in the hospital and a nurse will take a medical history. You will be given a hospital gown to wear for surgery.
Your knee will be cleaned prepared for surgery. An ice pack may be put onto your knee. Your anaesthetist may give you a pre-medication to help you relax before going to surgery. The surgery is done in a sterile (ultra-clean) operating theatre.
The surgery is usually done under general anaesthesia and a nerve block may be added after discussion between yourself and the Anaesthetist. The duration of the surgery varies depending on what else needs to be done at the time of surgery (meniscal repair, cartilage repair, and other ligaments) but is usually between 1 and 2 hours.
PROCEDURE
The procedure that we follow in an acute injury, is to do a biological ACL reconstruction. This is done as arthroscopic surgery (keyhole) with as little soft tissue damage as possible. As little of your original torn ACL is removed. One of your hamstring tendons (there are 4) is harvested and used as a graft to reconstruct the torn ACL. This hamstring tendon is then placed through the torn ACL and secured in the femur (with a button) and in the tibia (with a bio-absorbable screw). Your original torn ACL then heals onto the reconstructed ACL conferring certain advantages (mainly a better feeling inside in the knee and aids healing). If any other damaged occurred at the time of injury in the knee, it is now also repaired.
Sometimes, the patient may have re-torn a previously reconstructed ACL or the hamstring tendons are not available. In this case then either a strip of tendon, with bone, is taken from underneath your cap, or allograft tendon (donor tendon) is used for the reconstruction.
POST OPERATION
You will be seen by a Physiotherapist in the recovery room who will tell you what you can and cannot do. They will get you up on crutches and when you are safe and ready, you may go home. You will then be followed up 2 or 3 days later in the practice and the wounds reviewed.
REHABILITATION AFTER SURGERY
After surgery, crutches are used as needed and weight bearing allowed as pain allows. As the pain subsides, you may put more weight on the leg unless instructed not to by the Surgeon. After surgery, exercise and rehabilitative therapy are required to strengthen the muscles and restore mobility. With this procedure, most athletes can return to their chosen sport at the same level.
- Keep in mind that if your ACL injury requires surgery, the soft tissue needs time to heal before exercise can begin. While in the hospital, patients start partial weight bearing with exercises to re-establish knee joint mobility and normal gait.
- A physical therapy program usually begins with range-of-motion and resistive exercises, then incorporates power, aerobic and muscular endurance, flexibility, and coordination drills.
- Finally, patients develop speed and agility through sport-specific exercise routines. A typical patient may begin to ride a bike at three months, start running at five to seven months, and return to competitive sports after eight to 12 months. Full recovery may take up to two years.
- The ultimate goal of ACL reconstructive surgery is to provide dynamic stability while maintaining full range of motion, so that athletes can return to competitive or recreational sports. Progress is assessed by the patient’s perception of how stable the knee feels and by comparing the strength and stability of the injured and uninjured knees.
In general, initially the most important aspect is to obtain full extension and full flexion (usually by week 6). A physical therapy program usually begins with range-of-motion and progressive resistive exercises, then incorporates power, aerobic and muscular endurance, flexibility, and coordination drills. Finally, patients develop speed and agility through sport-specific exercise routines. A typical patient may begin to ride a bike at three months, start running at five to seven months, and return to competitive sports after eight to 12 months. Full recovery may take up to two years.
RETURN TO SPORTS
The goal of rehabilitation is to return you to your sport or activity as soon as is safely possible. If you return too soon, you may worsen your injury, which could lead to permanent damage. Everyone recovers from injury at a different rate. Your return to activity is determined by how soon your ACL injury recovers, not by how many days or weeks it has been since your injury occurred. It also depends on how serious the injury is. Instances where reconstructive surgery is required will obviously create a longer recovery period than patients with a strain or anterior knee pain.
The ultimate goal of ACL reconstructive surgery is to provide dynamic stability while maintaining full range of motion, so that athletes can return to competitive or recreational sports. Progress is assessed by the patient’s perception of how stable the knee feels and by comparing the strength and stability of the injured and uninjured knees.